 United States
United States
Getting Started With CRRT
Build a CRRT program tailored for your specific ICU needs.
Building a CRRT program for your ICU
Talk to our team of clinical specialists to explore your options to build a CRRT program and discover why we will be your trusted expert and partner throughout the process.
Helping you every step of the way
A successful CRRT program starts with a CRRT champion or committee and incorporates several key elements.11
We are here to help step by step, as you:
Step 1. Secure the devices and solutions you need
Step 2. Create policies to manage therapy
Step 3. Create standardised protocols for CRRT in your ICU
Step 4. Educate and train your physicians and nurses
Step 5. Monitor patient data to adjust therapy
A podcast series to help you get started
So many questions arise when starting to think about adding a CRRT program to your ICU. In this series of podcasts developed in collaboration with KDIGO, listen to experts discuss relevant parameters for when to offer, start, and stop CRRT therapy in critically ill patients.



Vantive Prismaflex and PrisMax are trademarks of Vantive Health LLC or its affiliates.
References
-
KDIGO Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl. 2012;2(1):1-138.
-
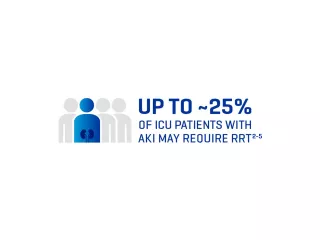
Bouchard J, Acharya, A, Cerda J, et al. A prospective international multicenter study of AKI in the intensive care unit. Clin J Am Soc Nephrol. 2015;10(8):1324-1331.
-
Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294(7):813–818.
-
De Corte W, Dhondt A, Vanholder R, et al. Long-term outcome in ICU patients with acute kidney injury treated with renal replacement therapy: a prospective cohort study. Crit Care. 2016;20:256.
-
Garzotto F, Ostermann M, Martín-Langerwerf D, et al. The dose response multicentre investigation on fluid assessment (DoReMIFA) in critically ill patients. Crit Care. 2016;20:196.
-
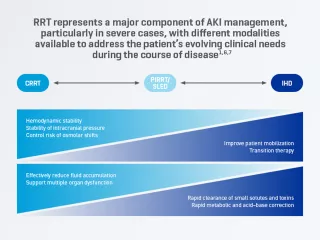
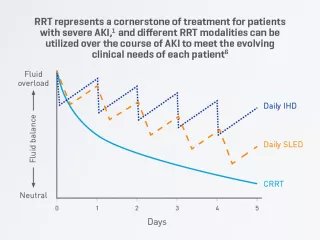
Ronco C, Ricci Z, De Backer D, et al. Renal replacement therapy in acute kidney injury: controversy and consensus. Crit Care. 2015;19(1):146.
-
Ostermann M, Joannidis M, Pani A, et al. Patient selection and timing of continuous renal replacement therapy. Blood Purif. 2016;42(3):224-237.
-
Augustine JJ, Sandy D, Seifert TH, Paganini EP. A randomized controlled trial comparing intermittent with continuous dialysis in patients with ARF. Am J Kidney Dis. 2004;44(6):1000-1007.
-
Bagshaw SM, Berthiaume LR, Delaney A, Bellomo R. Continuous versus intermittent renal replacement therapy for critically ill patients with acute kidney injury: a meta-analysis. Crit Care Med. 2008;36(2):610-617.
-
Fieghen HE, Friedrich JO, Burns KE, et al. The hemodynamic tolerability and feasibility of sustained low efficiency dialysis in the management of critically ill patients with acute kidney injury. BMC Nephrol. 2010;11:32.
-
De Becker W. Starting up a continuous renal replacement therapy program on ICU. In: Ronco C, Bollomo R, Kellum JA, eds. Contributions to Nephrology: Acute Kidney Injury. Basel, Karger; 2007:185-190.