 United States
United States
PrismaLung+ Filterset
A blood-gas exchanger on the PrisMax system for expanded treatment possibilities
Maximise ECCO2R performance
The PrismaLung+ blood-gas exchanger was specifically designed to enable CO2 removal with therapy-specific software on the PrisMax system. Combined with the TherMax blood warmer, the PrisMax system can help providers treat patients more confidently.
The PrismaLung+ blood-gas exchanger is intended for patients with increased levels of CO2 in their blood and with a body weight greater than or equal to 30 kg (66 Ib).1
Compatible Products
Acute Therapy Systems
CRRT Solutions
Filtersets & Catheters
Digital Solutions
ECCO₂R
Deliver stand-alone ECCO2R to support management of acute respiratory dysfunction.
ECCO₂R and CRRT combined
Combine therapies to support management of acute respiratory dysfunction and acute kidney injury.
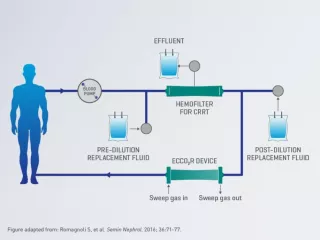
ECCO₂R, CRRT and blood purification for sepsis management simultaneously
Add blood purification for sepsis management to simultaneously support management of acute respiratory dysfunction and AKI in patients who may benefit from removal of endotoxins and inflammatory mediators – all with one vascular access point.
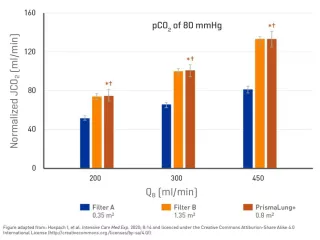
Optimise CO₂ removal with smaller membrane for risk management
The PrismaLung+ blood-gas exchanger delivers CO2 removal equivalent to that of a device with a larger surface area, while addressing risks that may be associated with extracorporeal therapies:
- Smaller membrane size to help reduce clotting risk
- Lower extracorporeal blood volume
An in vitro study shows that at the same blood flow rates and the same initial PaCO2 levels, the PrismaLung+ blood-gas exchanger (0.8 m2) provides similar CO2 removal rate performance when compared to a much larger membrane.7
Vascular access performance
By operating at blood flow rates similar to CRRT and using the same vascular access, the PrismaLung+ blood-gas exchanger limits the invasiveness of ECCO2R therapy compared to mid-flow ECCO2R and vv-ECMO. The PrismaLung+ blood-gas exchanger works with any brand catheter, and can be used with Vantive’s GamCath GDHK-1320 catheter, which has demonstrated one of the best access and return pressure performances at various blood flow rates when compared to other brands and designs including bigger catheter sizes (13, 14 and 15 FR).8
- With the PrismaLung+ blood-gas exchanger, operating blood-flow rates do not exceed 450 ml/min1 allowing ECCO2R to be performed using 13FR catheters, which are typically used for CRRT
- ECCO2R and CRRT can be run simultaneously using a single catheter, avoiding the need for multiple access sites
- The PrismaLung+ blood-gas exchanger with the PrisMax system allows the combination of ECCO2R with CRRT and blood purification for sepsis management in one extracorporeal circuit, thus reducing the total extracorporeal blood volume compared to running the therapies independently
Maintain patient blood temperature6
When integrated with the PrisMax system, the PrismaLung+ blood-gas exchanger uses the TherMax blood warmer to provide an advanced source of support for efficient and easy patient blood warming. Automatic blood heating adjustment helps meet the prescribed return blood temperature independently from blood flow rates and therapy interruptions.
Optimised ECCO₂R delivery with smart efficiencies
Integrate ECCO2R therapy into an existing CRRT setup with the PrismaLung+ blood-gas exchanger on the PrisMax system and reduce the need for additional capital expenditure and monitor maintenance while minimising staff training requirements.
Reduce the need for additional investments and monitor maintenance
Run all therapies (CRRT, TPE, ECCO2R, blood purification for sepsis management) and modalities (SCUF, CVVH, CVVHD, CVVHDF) using just one monitor with the PrisMax system.
Optimise staff workload and training
Streamline ECCO2R treatment setup with step-by-step software guidance through the intuitive PrisMax interface. Providing a setup and implementation routine similar to CRRT enables easy integration of the new therapy with limited training effort.
The PrismaLung+ blood-gas exchanger is easily added to the CRRT set, and the whole set is automatically one-step primed which means interactions during setup is similar to CRRT.
Enhance overall treatment accuracy
Help improve patient fluid balance accuracy with Vantive’s patented software algorithm estimating normal phenomenon of water evaporation during ECCO2R treatment.6



Contact Us
Speak with a Vantive representative to ask questions and learn how we can help you address challenges in your ICU.
References
-
PrismaLung+ Indication for Use. 2019.
-
Fanelli V, Ranieri MV, Mancebo J, et al. Feasibility and safety of low-flow extracorporeal carbon dioxide removal to facilitate ultra-protective ventilation in patients with moderate acute respiratory distress sindrome. Crit Care. 2016;20:36.
-
Schmidt M, Jaber S, Zogheib E, Godet T, Capellier G, Combes A. Feasibility and safety of low-flow extracorporeal CO2 removal managed with a renal replacement platform to enhance lung-protective ventilation of patients with mild-to-moderate ARDS. Crit Care. 2018;22(1):122.
-
Winiszewski H, Aptel F, Belon F, et al. Daily use of extracorporeal CO2 removal in a critical care unit: indications and results. J Intensive Care. 2018;6:36.
-
Combes A, Fanelli V, Pham T, Ranieri VM; European Society of Intensive Care Medicine Trials Group and the “Strategy of Ultra-Protective lung ventilation with Extracorporeal CO2 Removal for New-Onset moderate to severe ARDS” (SUPERNOVA) investigators. Feasibility and safety of extracorporeal CO2 removal to enhance protective ventilation in acute respiratory distress syndrome: the SUPERNOVA study. Intensive Care Med. 2019;45(5):592-600.
-
PrisMax Operator’s Manual. 2020; AW8046.
-
Hospach I, Goldstein J, Harenski K, et al. In vitro characterization of PrismaLung+: a novel ECCO2R device. Intensive Care Med Exp. 2020;8(1):14.
-
Vantive internal documentation. In-vitro Flow Comparison for CRRT Catheter. 2019.