 United States
United States
Expanding to Multi-Organ Support
Expand treatment possibilities for your patients by delivering single or combined multi-organ support therapies simultaneously on one device

Multi-organ dysfunction in the ICU
Multi-organ dysfunction is common in the ICU and can affect ~25-30% of critically ill patients.5,6
Deliver therapies simultaneously using a single vascular access
Management of multi-organ dysfunction is complex, requiring an integrated approach of pharmacologic and organ support therapies to both support individual organs and manage the effects of organ crosstalk.7 Clinicians can provide multi-organ support therapies using a single vascular access, helping to minimise the invasiveness of treatment8-10 and reduce the risk of infection for patients with multi-organ dysfunction.11-13 Furthermore, 90% of healthcare professionals have said that using a single system for multi-organ dysfunction would drive efficiencies for their hospital system.14
Expand
The integrated Vantive acute therapies portfolio expands treatment possibilities for patients with multi-organ dysfunction, helping clinicians to provide quality care.
Personalise
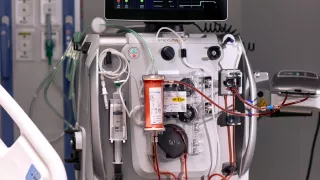
Simultaneous delivery of CRRT and other organ support therapies is possible with the PrisMax system, enabling personalised treatment through a single vascular access.17,18





Vantive, Oxiris, PrisMax and PrismaLung+ are trademarks of Vantive Health LLC or its affiliates.
References
-
Marshall JC. The multiple organ dysfunction syndrome. In Surgical Treatment: Evidence-Based and Problem Orientated. 2001. Accessed November 2021. Available at: https://www.ncbi.nlm.nih.gov/books/NBK6868/.
-
Batlle D, Soler MJ, Sparks MA, et al. Acute kidney injury in COVID-19: emerging evidence of a distinct pathophysiology. J Am Soc Nephrol. 2020;31(7):1380-1383.
-
Ronco C, Reis T, Husain-Syed F. Management of acute kidney injury in patients with COVID-19. Lancet Respir Med. 2020;8:738-742.
-
Husain-Syed F, Slutsky AS, Ronco C. Lung-kidney cross-talk in the critically ill patient. Am J Respir Crit Care Med. 2016;194(4):402-414.
-
Vincent JL, Sakr Y, Sprung CL, et al. Sepsis in European intensive care units: results of the SOAP study. Crit Care Med. 2006;34(2):344-353.
-
Vincent JL, Lefrant JY, Kotfis K, et al. Comparison of European ICU patients in 2012 (ICON) versus 2002 (SOAP). Int Care Med. 2018;44(3):337-344.
-
Ronco C, Ricci Z, Husain-Syed F. From multiple organ support therapy to extracorporeal organ support in critically ill patients. Blood Purif. 2019;48(2):99-105.
-
Consales G, Zamidei L, Turani F, et al. Combined renal-pulmonary extracorporeal support with low blood flow techniques: a retrospective observational study (CICERO Study). Blood Purif. 2022;51(4):299-308.
-
Allardet-Servent J, Castanier M, Seignouret T, et al. Safety and efficacy of combined extracorporeal CO2 removal and renal replacement therapy in patients with acute respiratory distress syndrome and acute kidney injury: the pulmonary and renal support in acute respiratory distress syndrome study. Crit Care Med. 2015;43(12):2570-2581.
-
Nentwich J, Wichmann D, Kluge S, Lindau S, Mutlak H, John S. Low-flow CO2 removal in combination with renal replacement therapy effectively reduces ventilation requirements in hypercapnic patients: a pilot study. Ann Intensive Care. 2019;9(1):3.
-
Joint Commission. Central line-associated bloodstream infections toolkit and monograph. Available at: https://www.jointcommission.org/-/media/tjc/documents/resources/hai/clabsi_monographpdf.pdf (accessed November 2021).
-
Dube WC, Jacob JT, Zheng Z, et al. Comparison of rates of central line-associated bloodstream infections in patients with 1 vs 2 central venous catheters. JAMA Netw Open. 2020;3(3):e200396.
-
Concannon C, van Wijngaarden E, Stevens V, Dumyati G. The effect of multiple concurrent central venous catheters on central line-associated bloodstream infections. Infect Control Hosp Epidemiol. 2014;35(9):1140-1146.
-
GLG Group. Prismaflex and Prismax Value Message Testing Market Research; 2021.
-
Takala J. Past and present challenges in ICU management. ICU Management. 2012;12(1):41-42.
-
Pierce LNB. Patient safety and production pressure: ICU nursing perspective. APSF Newsletter. Spring 2001.
-
PrisMax Operator’s Manual. March 2021.